Mortality and Case Rate
The Lethality and Case Count of COVID-19 is not much higher than a medium to moderately severe influenza.
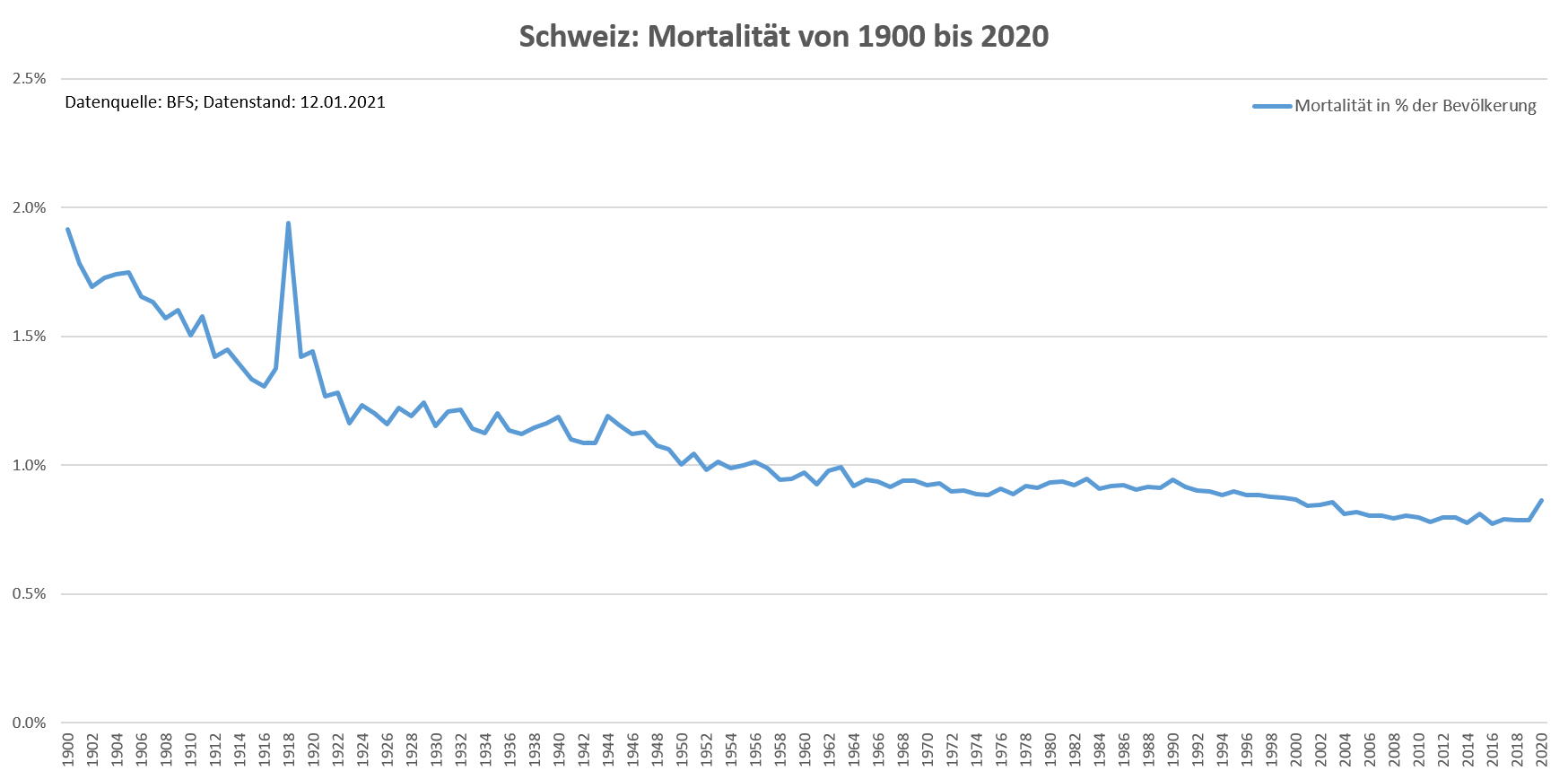
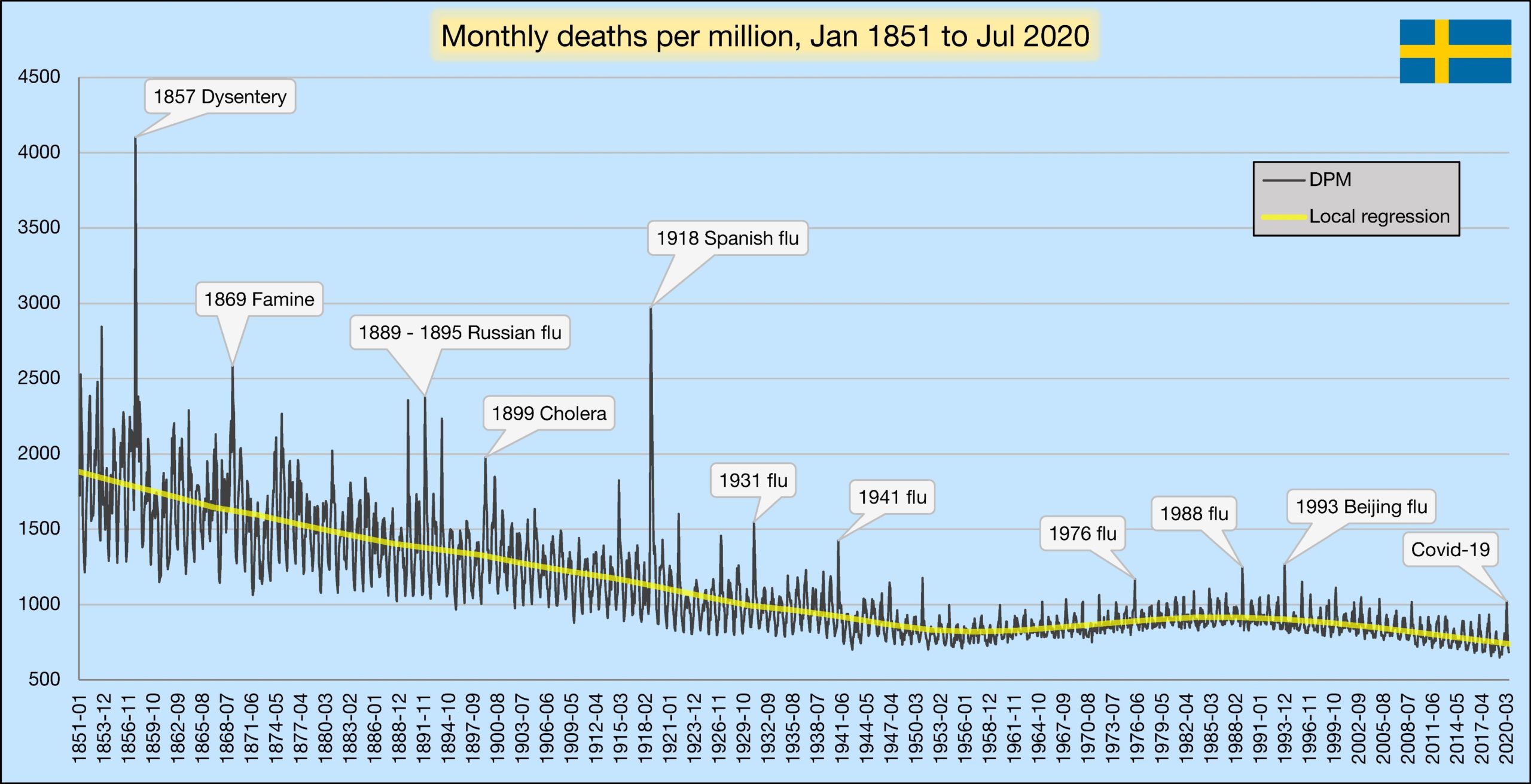
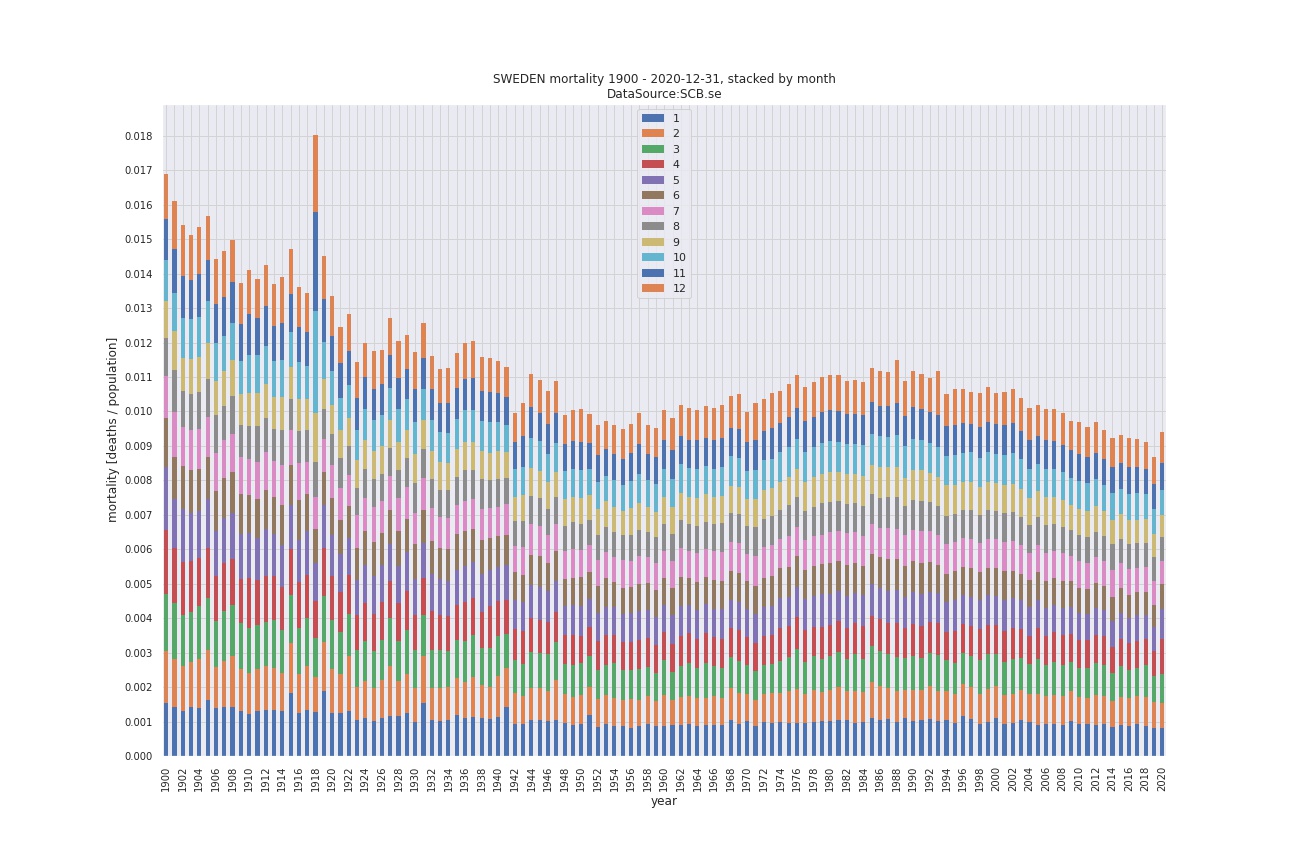
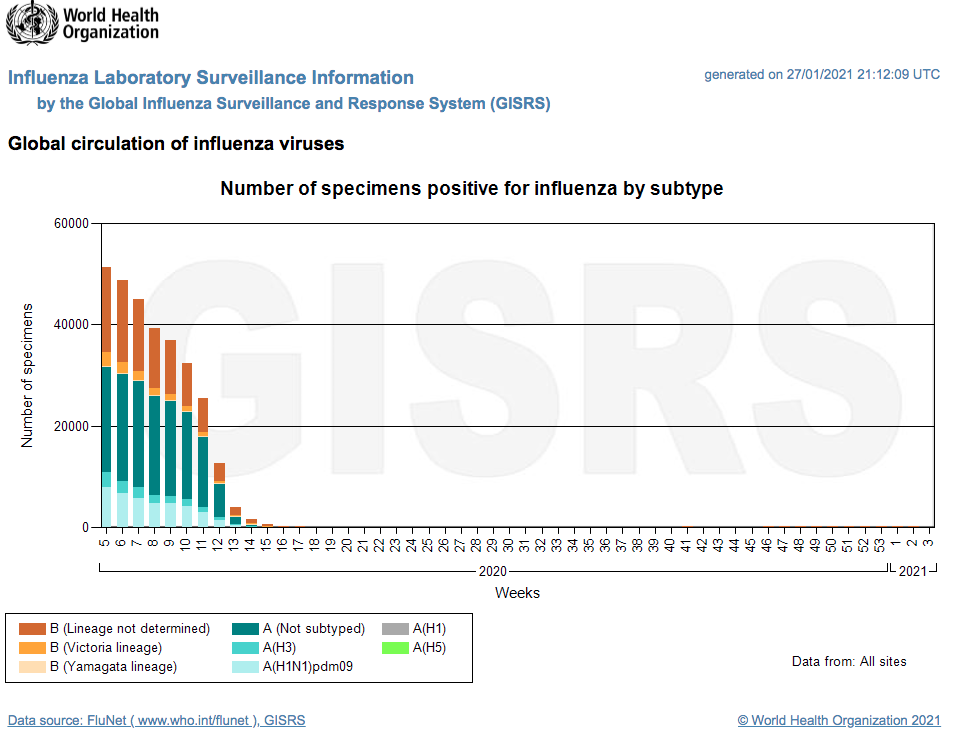
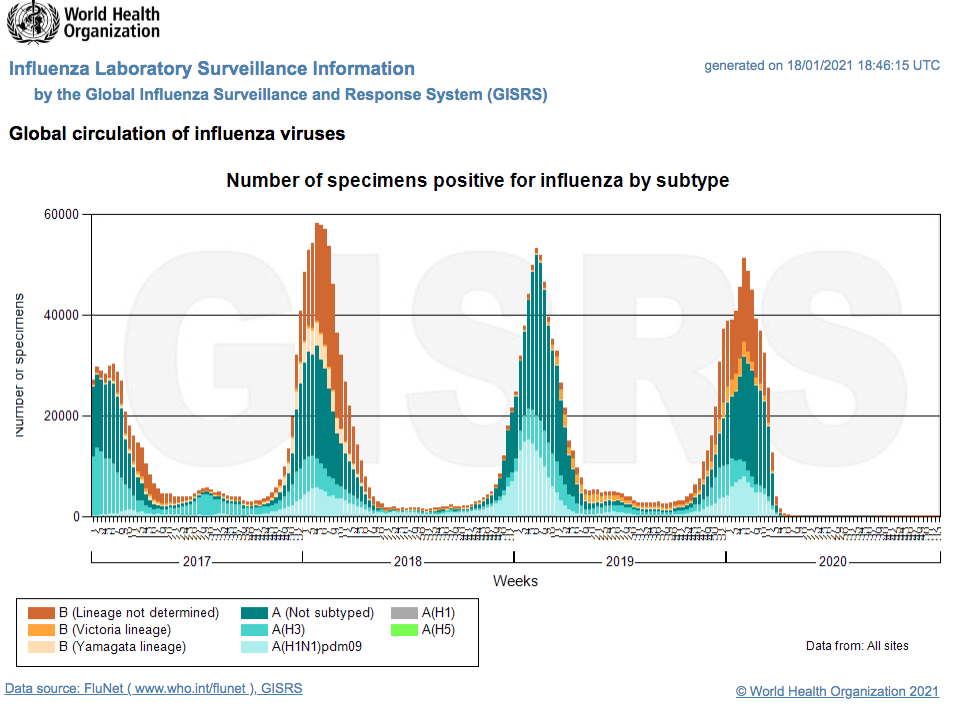
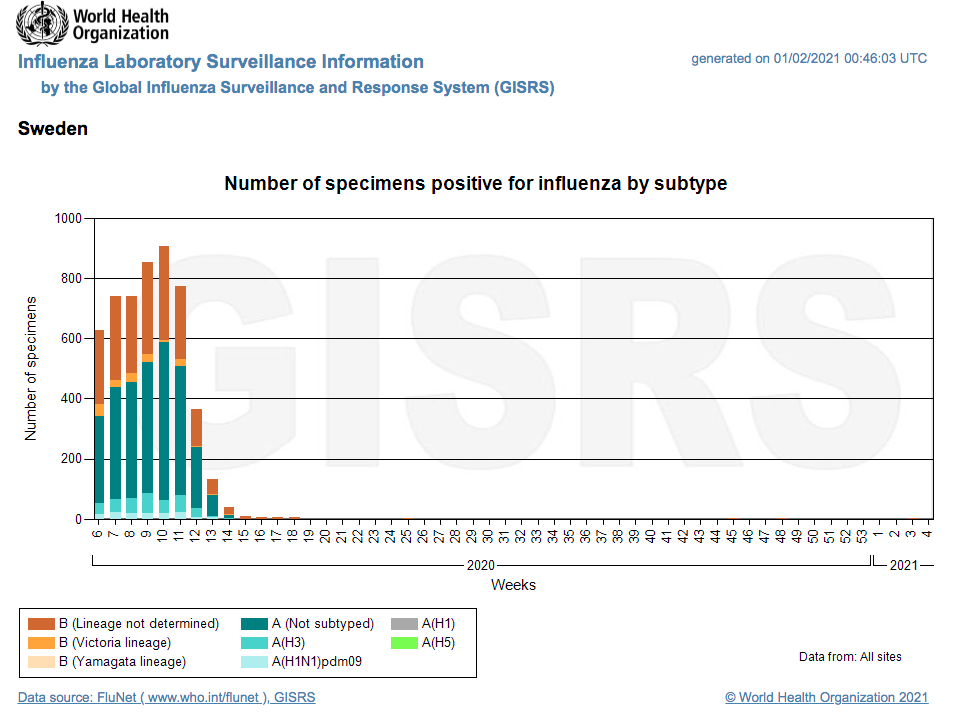
FLU
Flu waves occur every year. Different viruses are involved, mainly influenza and corona viruses.
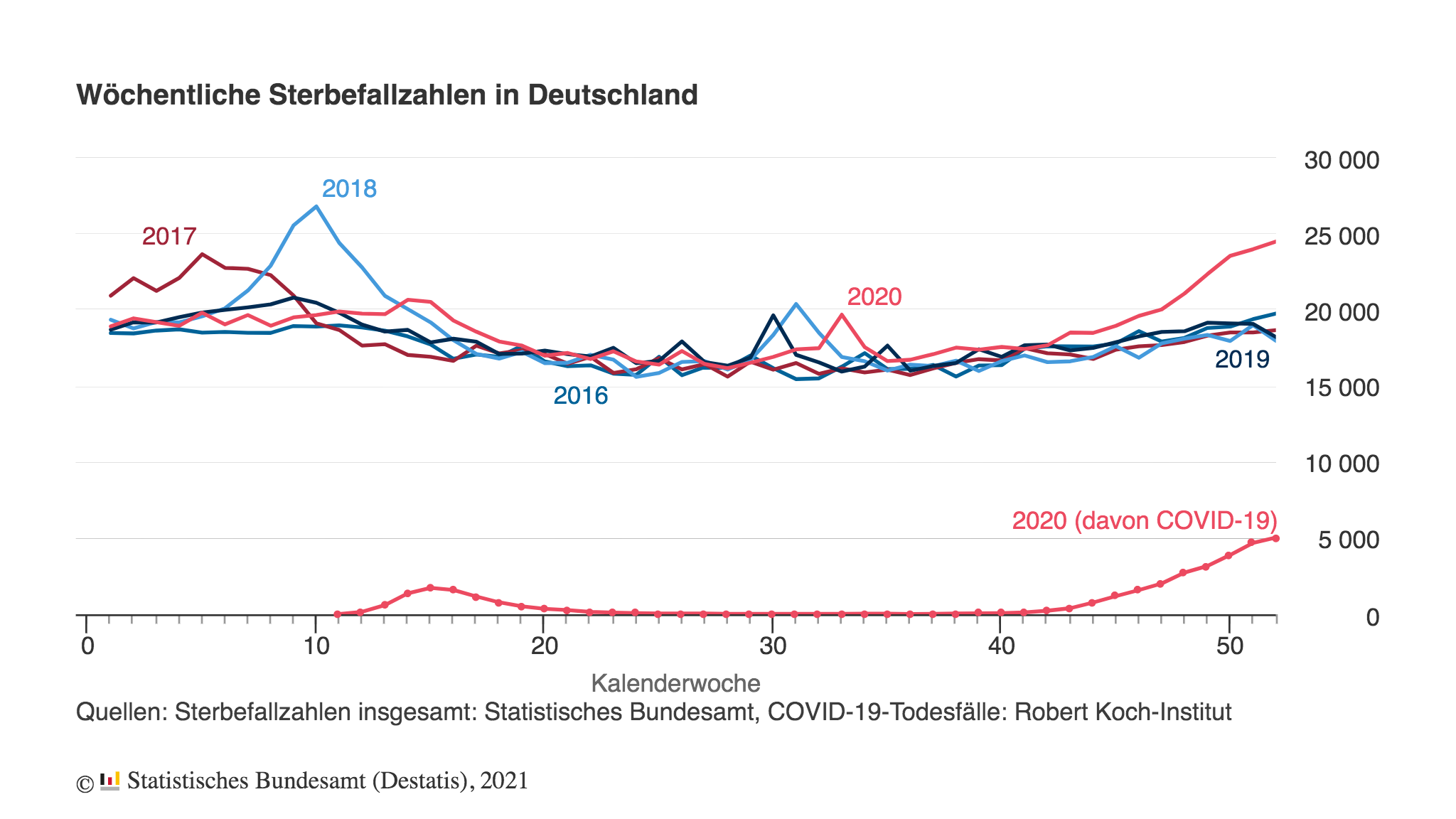
Normal case mortality with influenza or corona viruses is 0.1-0.2% sometimes like in 2017/2018 up to 1%.
COVID-19
October 2020
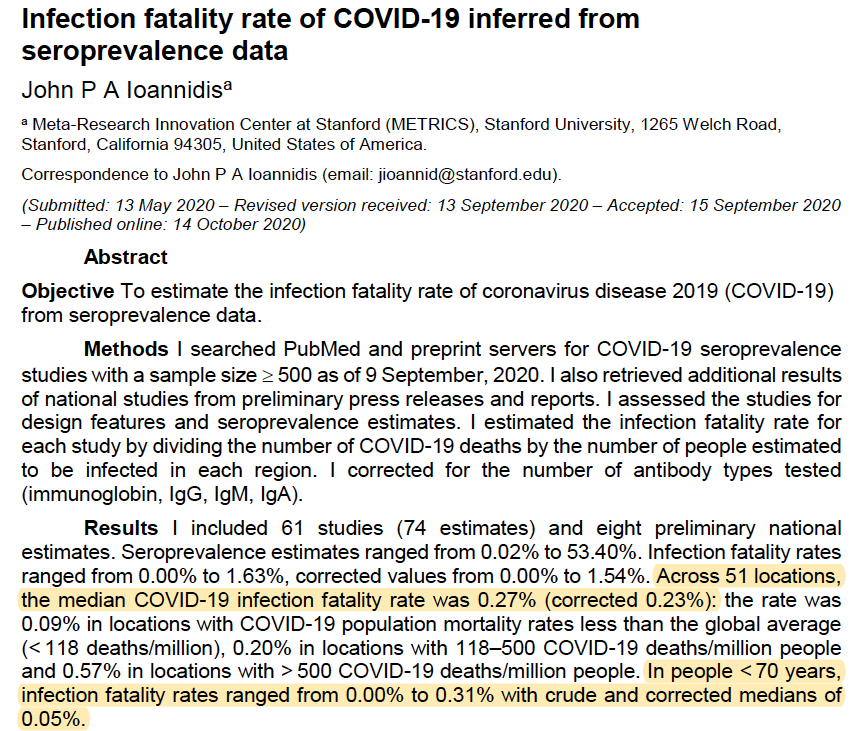
Bulletin of the World Health Organization / Infection fatality rate study by Prof. Ioannidis, Stanford University
Median COVID-19 infection fatality rate was 0.27% (corrected 0.23%)
People younger than 70 years, infection fatality rates ranged from 0.00% to 0.31% with crude and corrected medians of 0.05%.
https://onlinelibrary.wiley.com/doi/10.1111/eci.13423
October 12, 2020
IPAK PHPI:
Americans in the age of 0- 19, 20-49 and 50 to 69 demographics are at extremely low risk of fatality due to COVID-19
September 2020
John P.A. Ioannidis:
The median COVID-19 infection fatality rate was 0.23%
Younger than 70 infection fatality rates range from 0.00% to 0.31% and a median of 0.05%
September 10, 2020
CDC COVID-19 Pandemic Planning Scenarios
The risk of dying of COVID-19 at an age below 65 years: 0.00003 to 0.05%, for 70+ is 0.054 and for over 80 years: 1-2%
Age-specific survival rates:
0-19 years old 99.997%
20-49 years old, 99.98%
50-69 years, 99.5%
70 years old or older 94.6%
https://www.cdc.gov/coronavirus/2019-ncov/hcp/planning-scenarios.html#table-2
This is just in the range of a moderately severe flu wave.
April 2020
According to the German Heinsberg study by Prof. Streeck, infection fatality rate for all is in the range between 0.24% and 0.26% maximum 0.36% and a mortality (based on population) of 0.06%.
Conclusion: Covid-19 is definitely NOT a killer virus but comparable to a moderately severe influenza.
…… find more information here.